

The use of nitrous oxide is recommended by the dentist and her staff to ease anxious nerves, however it only works when the child is actively breathing it. If they are not breathing it, and crying, it will not help to calm them. When it is breathed well, it will create some lessening of pain and sensitivity, but it won't take away all pain, so numbing with anesthetic is still necessary in most instances in addition to nitrous oxide. Nitrous oxide will create a very calm child who is much less aware of what is going on, when it is breathed well. While a patient is on nitrous oxide, they will still be fully conscious and awake. It is important not to eat a large meal prior to using nitrous, as it can cause upset tummies in some after having a big meal.
Numbing is an important process when getting a cavity filled. This means that your child will experience some discomfort while the shot is being administered. Certain areas of the mouth such as the front and palate are very sensitive. We always try to minimize pain from an injection with the use of nitrous oxide, distraction techniques, tv, and the topical anesthetic, but in some instances, depending on the location and your child's own pain tolerances, they will still feel the shot. Also, depending on how many teeth or areas of the mouth are being worked on, multiple injections may have to be performed, to numb the important nerves for the teeth being treated. So, it's not typically just one shot for one tooth, and may be several if multiple teeth are being treated. It is important not to overly scare a child before arriving to the dentist for their procedure. Sometimes less information can be better. The good news is that most shots do not take long, and once this important part is over, the remaining dental procedure is pain free.
After the tooth or teeth are asleep, a dental drill is used to remove the soft areas of cavity present in the tooth. The drill has a stream of water and creates a buzzing noise. The buzzing noise can be loud to a child as well as the vibrations against the cavity and tooth structure. It is important to know, that sometimes sounds, and vibrations unknown to a child, can seem like pain, when really it is just pressure or sensations they hear or feel that are not actually pain.
Once the dentist starts to drill on the tooth, this means the procedure will have to be finished, since the tooth will now have missing tooth structure. Therefore, if the child is crying or unable to understand, what is going on once the procedure is started, it will need to be finished. Sometimes this involves staff or parents having to hold a patient for safety to finish the necessary procedure.
Sometimes, when a cavity is treated; the dentist may find that the cavity is larger or occupies more of the tooth than what we thought. Sometimes the adjacent tooth can also have a cavity that may not have shown up on the x-ray but is visible when the opposing tooth surface has been opened up.
Getting a cavity filled is a medical procedure, and while dentistry has advanced, our office does everything we can to minimize this discomfort, but there are still parts of it that can be uncomfortable.
Self-induced soft tissue injury caused by lip and cheek-biting is an unfortunate complication of local anesthetic used in the mouth and is usually self-limiting and heals without complications, although bleeding may result. The frequency of self-induced soft tissue injury is higher when only one side is anesthetized. To help avoid the possibility of soft tissue injury, patients and their parents or caregivers need to be especially watchful and not allow the patient to bite, suck, or scratch on their lip, cheek, or tongue, and do not allow them to eat food while the anesthesia persists (still numb). If an injury does occur, it is best to cleanse the mouth with either OTC Peroxyl rinse, or warm salt water. If necessary, Tylenol or Motrin can be used to alleviate pain while the area is healing.

FOR SILVER CAPS: The area around the dental work will be numb for 2 hours after the dental work. Once the area wakes up, gums around crowns will be tender, irritated, and sore for up to a week following the dental procedure. To help relieve tenderness and irritation, over the counter Tylenol or children's Motrin can be given every 4-6 hours for the days following the work. A softer diet with mild foods is best at first, and after the numbness has worn off. Milkshakes, Jell-O and soup are good foods to start with. Also, it is important to keep the gums and teeth cleaned, so bacteria and food doesn't become impacted into the irritated gums. Brush gently with small circles around the gums and caps, with toothpaste. Peroxyl, Listerine, or Crest Pro-Health mouth rinses can be used to swish with, or a Q-tip dipped in the rinse can be used to help keep the areas cleaned. Orabase tooth numbing gel can be applied around the irritated gums as well, to temporarily numb the tissue. It takes time for the gums and teeth to heal, just like getting used to wearing a new pair of shoes.
FOR WHITE FILLINGS: The area around the dental work will be numb for 2 hours after the dental work. Avoid eating until the numbness wears off. Once the area awakes, the gums around the dental work may be tender, irritated, and sore for up to a week following the dental procedure. To help relieve tenderness and irritation, over the counter Tylenol or children's Motrin can be given every 4-6 hours for the days following the work. A softer diet with mild foods is best at first, and after the. numbness has worn off. Milkshakes, Jell-O and soup are good foods to start with. Also, it is important to keep the gums and teeth cleaned, so bacteria and food doesn't become impacted into the irritated gums. Brush gently with small circles around the gums with toothpaste. Peroxyl, Listerine, or Crest Pro-Health mouth rinses can be used to swish with, or a Q-tip dipped in the rinse can be used to help keep the areas cleaned. Orabase tooth numbing gel can be applied around the irritated gums as well, to temporarily numb the tissue.
FOR SEALANTS: At first your child may complain of a funny taste. Sealants are applied using several steps which tend to leave a sour or "yucky" taste. This is normal and will go away after the child eats or drinks something. Your child may eat and drink following the sealant procedure, as long as they avoid sticky and hard foods such as Laffy Taffy, caramel, jawbreakers, etc. Sealants will be high upon gentle closing at first, but over the next few weeks, the sealants adjust to the tooth, filling in the voids and crevices within the tooth.
FOR SPACERS, THUMB SUCKING APPLIANCES, OR OTHER APPLIANCES:
Since the appliances are held into place with dental glue, your child may complain of a funny flavor. This funny flavor will go away with time. In addition, the gums and teeth may be sore around the appliance for up to a week. The appliances are meant to squeeze the teeth, as they are holding space. Also, they are embedded into the gums and may cause a temporary tenderness and irritation to the gums. To help relieve tenderness and irritation, over the counter Tylenol or children's Motrin can be given every 4-6 hours for the days following the work. A softer diet with mild foods is best at first. Milkshakes, Jell-O and soup are good foods to start with. Also, it is important to keep the gums and teeth clean, so bacteria and food doesn't become impacted into the irritated gums around the appliances. Appliances provide and extra niche for bacteria and plaque to hide, so it is even more important to keep these clean. Brush gently with small circles around the gums and appliances with toothpaste. Peroxyl, Listerine, or Crest Pro-Health mouth rinses can be used to swish with or a Q-tip dipped in the rinse can be used to help keep the areas cleaned. Orabase tooth numbing gel can be applied around the irritated gums as well, to temporarily numb the tissue. It takes time for the gums to heal around an appliance, just like getting used to wearing a new pair of shoes. It is best to avoid sticky and hard foods for the duration of the appliance. This means to avoid sticky candies and very crunchy hard foods. If the spacer becomes loose or comes out, out it into a Ziploc bag and call to make an appointment as soon as you can.
Your Pediatric Dentist is an important part of the team approach to your child’s total health. Good oral health is an important part of total health. When helping children and adolescents, a pediatric dentist works closely with Pediatricians, other physicians and other dental specialists Including orthodontists. All young people are served best through this team approach. Papillion Pediatric Dentistry is an important part of your child’s health team. Why should you take your children and adolescents to a Pediatric Dentist? No one person can be an expert in everything. Think how in business there are people who have specialized in different areas, such as engineers, sales people, accountants, and production workers. You would not go to the accountant to ask them to design a product nor would you ask the engineer to prepare the monthly financial statements. Why, because each is an expert in the specialty in which they were trained. And while the engineers and accountants all have some knowledge about each other’s field they certainly are not experts in the other’s specialty. This is also true in the medical and dental field. All dentists and medical doctors receive basic training in the general art of dentistry or medicine but are not experts in every aspect of dentistry or medicine. Like specialties in any field, you would not go to a doctor specializing in heart surgery to fix a broken foot but one specializing in orthopedics and you would not take your grandmother to a Pediatric Dentist but a dentist that is experienced in treating older adults. Pediatric dentists are the pediatricians of dentistry. Pediatric dentistry is the specialty of dentistry that focuses on the oral health and unique needs of young people. After completing college and a four-year dental school curriculum, two additional years of rigorous training (Dr. Bennett’s was hospital based) is required to become a pediatric dentist. This specialized program of study and hands-on experience prepares pediatric dentists to meet the unique needs of infants, children and adolescents, including persons with special health care needs.
There has been an increasing trend in outpatient procedures that involve patient sedation in an office environment and unfortunately, several tragedies has brought this to the forefront. As a result, the American Academy of Pediatric Dentistry (AAPD) and the American Academy of Pediatrics (AAP) announced updated joint recommendations for all medical and dental practitioners regarding the monitoring and management of pediatric patients during and after sedation while in a non-hospital setting. While many practitioners are comfortable providing sedation in an office environment, Dr. Bennett believes that better care can be provided in a hospital setting. While all medical procedures carry risk, Dr. Bennett believes that those patients in need of general sedation are best cared for in the hospital environment under the care of an MD Anesthesiologist who specializes in general sedation and not in a riskier office setting. This team approach allows Dr. Bennett to totally focus her attention on her dental procedures while the anesthesiologist monitors the child while under general sedation. Dr. Bennett has Operating Room privileges at Boys Town National Research Hospital - West. Several times a week she provides care in the hospital operating room to those patients unable to tolerate treatment in the traditional dental office setting without general sedation. Patients requiring these services are usually the infant or young child with extensive dental restorative needs and the medically and mentally compromised patient with special needs.
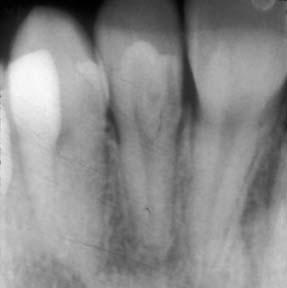
We follow the American Academy of Dentistry and American Academy of Pediatric Dentistry guidelines for taking dental X-Rays. Dental x-rays will be taken as needed during their routine cleaning appointments to check for cavities in between their teeth, survey erupting teeth, diagnose bone disease, evaluate the results of an injury, or plan orthodontic treatment. We will always minimize your child’s radiation exposure by prescribing X-Rays on an individual basis which depends on your child’s individual risk factors for oral disease. Your child will also wear a lead body apron during the process. If you have any concerns about X-Rays for your child, please discuss them with our staff.
The last and best part of your child’s routine cleaning appointment is a thorough examination with Dr. Bennett as she takes the time to get to know every child and form lasting relationships with your child. The exam includes visual examination of your child’s teeth and mouth, “counting” and “exploring” your child’s teeth and talking to your child about their teeth and hygiene. If your child has decay or other problems requiring treatment, the dentist will discuss them with you and a treatment appointment will be set for a later date.
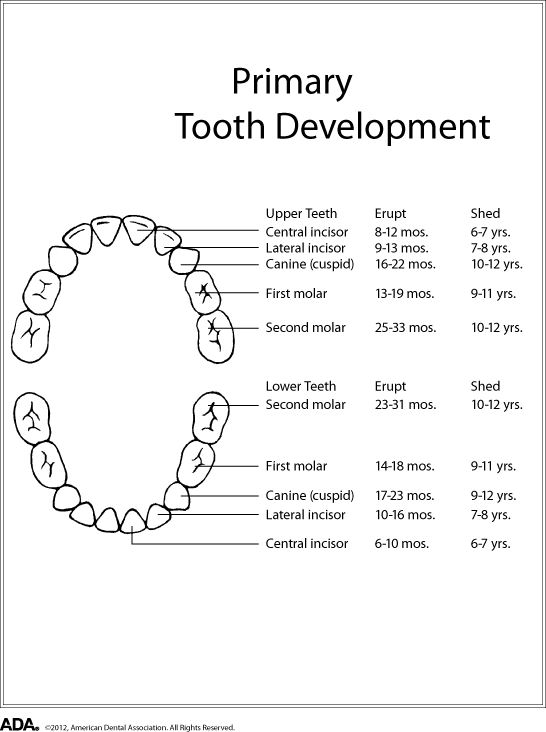
At about 6-8 months, the two lower front teeth (central incisors) will erupt, followed shortly by the two upper central incisors. The remainder of the baby teeth appears during the next 18 to 24 months. At 2 to 3 years, all 20 of the primary teeth should be present.
The pace and order of their eruption may vary, so don’t be alarmed if some teeth are a few months early or late. All children have unique eruption patterns.
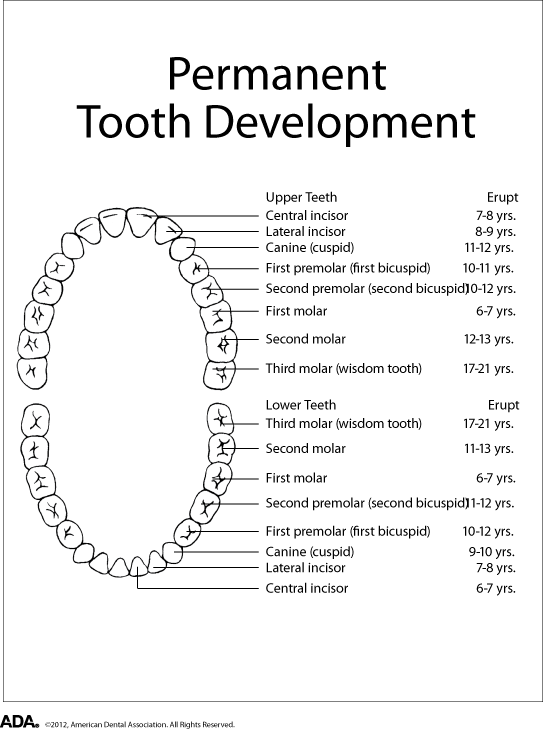
The first permanent teeth begin to erupt at about age five to six and include molars behind the back baby teeth along with lower central incisors. Some permanent teeth replace baby teeth and some don’t. This process will continue until approximately age fourteen.
The pace and order of their eruption may vary, so don’t be alarmed if some teeth are a few months early or late. All children have unique eruption patterns.
Your child’s general health is affected by the health of their teeth and gums. Primary, or "baby," teeth are important for many reasons. Not only do they help children speak clearly and chew naturally, they serve as space holders for the permanent teeth as they aid in forming a path that permanent teeth can follow when they are ready to erupt. We are often asked, Why we put fillings in baby teeth when they will fall out anyway? Neglected cavities create problems that affect the development of permanent teeth. Neglected cavities progress to the core of the tooth and eat away at the nerve. The tooth becomes painful and the nerve becomes inflamed, eventually dying. This creates an abscess that often results in the loss of the tooth and serious damage to the permanent tooth growing below. Some severe cases require emergency hospitalization.
Brown or missing teeth often affect the development of self-esteem. A beautiful smile enhances self confidence regardless of age. Research shows that children with numerous cavities are often underweight because eating begins to hurt. As a result, they limit food choices, disrupting proper nutrition.
Children learn to talk using their primary teeth. Research shows that, because most speech skills are already formed by the age of seven, children who lose their primary front teeth too early often need speech therapy.
Your child’s general health is affected by the health of their teeth and gums.
Also known as Early Childhood Caries or Nursing Caries, Baby Bottle Tooth Decay is caused by over exposure to sugary liquids. It is usually caused by putting a baby to bed with a bottle containing milk, juice, or soda, nursing babies on demand through the night, or allowing toddlers to graze with a sippy cup. This condition often destroys primary teeth, creating a need for major dental treatment. In addition, it will eventually damage your child’s permanent teeth if left untreated.
You can prevent this by following a few simple guidelines:
1) Never allow your child to fall asleep with a bottle containing milk, formula, breast milk, fruit juices, or any sweetened liquids.
2) Never give your baby a pacifier dipped in sugar or honey.
3) Only allow water in bottles and sippy cups used for grazing.
4) Wipe your baby’s gums with a clean gauze pad after each feeding, and begin brushing as soon as the first tooth appears.
5) Encourage children to drink from a regular cup by their first birthday.

The American Academy of Pediatric Dentistry and American Academy of Pediatrics recommends every child see a dentist by the time their first tooth erupts and no later than their first birthday. Establishing a dental home early will encourage healthy habits that last a lifetime and ensure that your child receives preventive care. Routine dental cleanings and exams are important for your child to maintain good oral hygiene and prevent tooth decay and disease. Your daily home care is also critical, but the professional cleanings remove mineralized plaque that can develop despite good brushing and flossing, particularly in areas that are difficult to reach. During the appointment, your child’s teeth will be polished and scaled to remove the plaque and tartar from the tooth surfaces and under the gum line. He or she will get to choose a fun toothpaste flavor like fruit or bubble gum before sitting back to watch a kid-friendly TV show overhead while their teeth are cleaned. The hygienist will spend time reviewing your child’s dietary intake and daily dental hygiene routines. She will encourage healthy eating habits and instruct proper brushing and flossing techniques at each checkup visit.
Positive attitudes and feelings toward the dental visit are encouraged. We strive to make each visit fun and have our patients leave happy. Your child will leave the office with a new cool toothbrush, dental floss and great flavored toothpaste as well as a token to put in our toy machine to get the prize of your choice.

Papillion Pediatric Dentistry focuses strongly on prevention and wants to help our patients grow up cavity-free. We strongly encourage you to have your child’s teeth sealed because it is one of the most effective and easy ways to help prevent tooth decay. Dental sealants act as a barrier to prevent cavities and can be applied to baby molars and adult premolars and molars. They should be applied as early as possible after the adult tooth erupts and before cavities get a chance to form. The chewing surfaces are the most likely areas to get cavities and toothbrush bristles cannot reach all the way into the depressions and grooves of back teeth. Sealants protect these vulnerable areas by “sealing out” plaque and food. Sealants generally last several years, and the cost of sealants is very low compared to getting cavities filled.

Sealants are a coating that is applied to the teeth to protect the grooved and pitted surfaces of back teeth. Most cavities start in the deep pits and grooves that naturally occur in teeth because a toothbrush is unable to reach into these tiny pits. The sealant therefore seals out any bacteria or cavity bugs from reaching into these tiny pits. Why is it important to protect baby teeth when they are just going to be lost anyway? The baby teeth in the back of the mouth will stay with a child until he or she reaches the ages of 10-13. A simple sealant procedure that can be done on a child at age 3-5, takes only a few minutes, and can prevent cavities, creating a healthy oral environment for the new teeth that come in during the teenage years. Sealants don’t require a shot and are not expensive. They are a great option for baby teeth!
A dental extraction, which is often referred to as getting a tooth pulled, is a common procedure performed by pediatric dentists. Extractions may be necessary due to extensive dental cavities causing pain or infection, dental trauma or for orthodontic reasons. Most extractions are easy and routine and can be performed within the comfort and familiarity of our office. If Dr. Bennett feels that the extraction is more complicated, your child may be referred to an Oral Surgeon. To ensure that your child has a pleasant experience we recommend both Nitrous Oxide (to help them relax) and a local anesthetic (to numb the area). Rarely will your child require stitches. The area will heal on its own. It is important that you monitor your child so that they do not bite their lip or tongue. If there is sustained bleeding at home, try placing cotton gauze over the extraction site and have your child bite firmly for 30 minutes. You may also wet a tea bag and have your child bite on it gently. The tannic acid will stop bleeding naturally within 15 minutes. Have your child keep their fingers out of their mouth. Your child may eat a soft diet as soon as the numbness wears off, avoiding acidic food and drinks, such as tomato sauce and orange juice. Do not drink from a straw for the first 48 hours. Brush the area carefully and gently. Your child should relax after surgery, as strenuous physical activity may increase bleeding. You may start rinsing with a warm salt-water solution after 24 hours. Make your own salt water by mixing 1 tsp (5 g) of salt in a medium-sized glass [8 fl oz (237 mL)] of warm water. Give your child Tylenol or Motrin as per label instructions to control any discomfort they may experience. If you have any concerns about pain, bleeding or healing, contact us immediately.
A cavity that involves the nerve (pulp) of the tooth may cause a child to experience intense pain. Although the pain may subside for a period of time using ibuprofen or antibiotics, it will return unless the tooth is properly treated. When the nerve of the tooth is infected, it must be treated to restore the child to good dental health.
A pediatric root canal procedure is referred to as a “pulpotomy.” The purpose of root canal treatment is to maintain the vitality of the affected tooth so that the tooth will not be lost early. Early loss of posterior (back) primary teeth may cause future problems with the eruption of permanent teeth. Therefore, it is best to avoid early loss of primary molars by properly treating the nerve of infected teeth with a pulpotomy. Dental caries (cavities) and traumatic injury are the main reasons for a tooth to require pulp therapy. The pulpotomy root canal procedure removes the infected pulp tissue within the crown of the tooth. A medication is placed to calm the nerve of the tooth and prevent bacterial growth. The pulpotomy is followed with a final restoration of a stainless-steel crown.
After the pulpotomy (root canal procedure) is complete; your child should feel much better. We expect all pain to subside either immediately or within a few days of the procedure.
A Fluoride treatment in the form of a varnish (a sticky coating which minimizes ingestion) will be applied to your child’s teeth at the end of each checkup visit or more often depending on their cavity risk. Your child will be able to eat and drink right away, just nothing hard or sticky or too hot for 4-6 hours. Fluoride is a safe and effective way to help your child’s teeth stay strong and cavity-free. We will also discuss optimal fluoride intake from all sources; i.e. Fluoridated water, toothpaste and mouth rinsing to help keep your child’s teeth strong while minimizing the risk of Fluorosis (white or brown spots) on their developing adult teeth.
Fluoride is a natural occurring compound. Fluoride compounds are components of minerals in rocks and soil. Water passes over rock formations and dissolves the fluoride compounds that are present, releasing fluoride ions. The result is small amounts of fluoride are present in all water sources. Many scientific studies have shown that fluoride is beneficial to teeth. However, too little or too much fluoride can be detrimental to the teeth. Little or no fluoride will not strengthen the teeth to help them resist cavities. Excessive fluoride ingestion by preschool aged children can lead to dental fluorosis, which is a chalky white to even brown discoloration of the permanent teeth. Many children often get more fluoride than their parents realize. Being aware of a child’s potential sources of fluoride can help parents prevent the possibility of dental fluorosis. Some of these sources are: Too much fluoridated toothpaste at an early age. The inappropriate use of fluoride supplements. Hidden sources of fluoride in the child’s diet. Two and three-year old’s may not be able to expectorate (spit out) fluoride-containing toothpaste when brushing. As a result, these children may ingest an excessive amount of fluoride during tooth brushing. Toothpaste ingestion during this critical period of permanent tooth development is the greatest risk factor in the development of fluorosis. Excessive and inappropriate intake of fluoride supplements may also contribute to fluorosis. Fluoride drops and tablets, as well as fluoride fortified vitamins should not be given to infants younger than six months of age. After that time, fluoride supplements should only be given to children after all the sources of ingested fluoride have been accounted for and upon the recommendation of your pediatric dentist. Certain foods contain high levels of fluoride, especially powdered concentrate infant formula, soy based infant formula, infant dry cereals, creamed spinach, and infant chicken products. Please read the label or contact the manufacturer. Some beverages also contain high levels of fluoride, especially decaffeinated teas, white grape juices, and juice drinks manufactured in fluoridated cities. Parents can take the following steps to decrease the risk of fluorosis in their children’s teeth: Use baby tooth cleanser on the toothbrush of the very young child. Place only a pea sized drop of children’s toothpaste on the brush when brushing. Account for all the sources of ingested fluoride before requesting fluoride supplements from your child’s pediatric dentist. Avoid giving any fluoride containing supplements to infants until they are at least 6 months old. Obtain fluoride level test results for your drinking water before giving fluoride supplements to your child.
When a tooth is lost prematurely due to cavities or trauma, a spacer is often recommended to hold the gap open for the adult tooth to erupt later when it’s ready. Space maintainers help prevent shifting and crowding of the adult teeth.
The Toothbrush - Care, Cleaning, Storage, and Replacement
Toothbrushing plays an important everyday role for personal oral hygiene and effective plaque removal, but appropriate toothbrush care and maintenance are also important considerations for sound oral hygiene. The ADA and the Council on Scientific Affairs provide the following toothbrush care recommendations: Do not share toothbrushes. Sharing a toothbrush could result in an exchange of body fluids and/or microorganisms between the users of the toothbrush, placing the individuals involved at an increased risk for infections. This practice could be a particular concern for persons with compromised immune systems or existing infectious diseases. Thoroughly rinse toothbrushes with tap water after brushing to remove any remaining toothpaste and debris. Store the brush in an upright position if possible and allow the toothbrush to air-dry until used again. If more than one brush is stored in the same holder or area, keep the brushes separated to prevent cross-contamination. Do not cover toothbrushes or store them in closed containers. A moist environment such as a closed container is more conducive to the growth of microorganisms than the open air. Replace toothbrushes at least every 3–4 months. The bristles become frayed and worn with use and cleaning effectiveness will decrease. Toothbrushes will wear out more rapidly depending on factors unique to each patient. Check brushes often for this type of wear and replace them more frequently if needed. Children’s toothbrushes often need replacing more frequently than adult brushes. Remember when replacing your child’s toothbrush to choose a proper toothbrush that reaches every surface of every tooth comfortably. Look for a toothbrush approved by the American Dental Association (ADA). Toothbrushes with small heads are best as they can help reach difficult to clean areas near the back of the mouth and between the tongue and lower molars. Bristles can be categorized as soft and medium. It is always recommended that you use a soft brush, so it is gentle on the gums and also remember to change your child’s brush after your child has been sick.
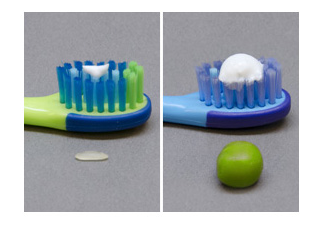
Following the most up-to-date guidelines by the American Dental Association and the American Academy of Pediatric Dentistry, you may start using a tiny smear of fluoride toothpaste as soon as the first baby teeth erupt. By 3 to 6 years of age, the amount should be increased to a pea-sized dollop. Parents should supervise brushing to ensure the proper amount of toothpaste is being used. Children naturally want to swallow toothpaste after brushing, and swallowing too much fluoride toothpaste can cause teeth to stain.
Just because your child is a teenager doesn’t mean they should stop seeing their pediatric dentist. Dentistry to meet the special needs of teens and adolescents is an important part of the specialized training for pediatric dentists. Growing doesn’t stop at childhood – teens experience important growth in their faces and jaws. Teens are also getting the last of their permanent teeth, and teeth that have just come through the gums are especially vulnerable to decay. Additionally, teenagers start becoming responsible for their own diet and nutrition choices, and it’s important that those choices contribute to good dental health.
We understand that often tooth color may be an aesthetic issue for adolescent patients and we offer safe and gentle bleaching to lighten the color of your child’s teeth. We encourage your teenage child or you to address any cosmetic concern you may have and will offer you a solution that meets your needs.
Parents are more likely to encourage mouth guards only for their sons and not for their daughters... are they right? Researchers have shown that there is a perceived notion that males are more likely to be involved in traditional contact sports. However, recent studies report that oral and facial injuries to female athletes exceed those in males! Which sports require mouth guards? Most parents believe that football, hockey and wrestling are sports that place children most at risk for oral and facial injury and therefore should have mandatory policies on mouth guards. However, most parents also perceived little need for mouth guards in basketball, baseball and soccer. But 19 percent of injuries occurred in basketball, 17 percent in baseball and 11 percent in soccer. Therefore, mouth guards should be used in all sports with the potential for contact and interaction between participants or an object. This includes football, hockey, wrestling, basketball, baseball, and soccer or any other activity that may result in a blow to the face or mouth. Why wear a custom mouth guard? Having a custom mouth guard specifically for your child will provide the best comfort and protection for your child’s smile. It will stay in place much better while your child is wearing it, making it easy for your child to talk and breathe. Please call 402-502-1256, to set up a time to have a custom-made mouth guard fabricated in time for your children’s sports. Are there different types of mouth protectors? Yes, there are three types of mouth protectors: Custom-fitted mouth protectors are made by Papillion Pediatric Dentistry for you personally. They are more expensive than the other versions, because they are customized and they offer a much better fit than anything you can buy off the shelf. Stock mouth protectors are inexpensive and come pre-formed. Unfortunately, they often don’t fit very well and are bulky and can make breathing and talking difficult. Boil and bite mouth protectors also can be bought at many sporting goods stores and may offer a better fit than stock mouth protectors. But, because they are designed to fit every mouth they never fit as good as a custom-made mouth protector. If you don’t follow the directions carefully you can wind up with a poor-fitting mouth protector that can irritate your children’s gums.
Yes, as soon as your child develops teeth that exhibit close contacts, flossing should begin. Toothbrushes cannot reach between the teeth, when tight contacts are present. The only way to remove plaque, food, and bacteria, is through flossing. Special flossers are available in the oral health section of most stores to help parents easily floss small children’s teeth. Be sure that your child visits the dentist regularly, brushes twice daily, begins a flossing routine, and uses a fluoride toothpaste to help strengthen the enamel. In addition, it is important to give children healthy food choices that are good for the teeth. These include fruits, vegetables, low-fat yogurt, and cheese. Remember... Floss – floss – floss!
Parents should continue to brush their children’s teeth until age 7-9 years of age. Studies have shown that children do not have the manual dexterity or the ability to brush their own teeth to prevent tooth decay until about that age. Usually, when children can tie their own shoes they should be able to brush on their own with limited supervision. Girls are usually able to master the task at a slightly earlier age than boys. Parents should always encourage children to try tooth brushing on their own, but this should be followed up with parental assisted brushing. The back teeth and around the gums are the easiest places for children to miss when brushing, and the most common places for cavities to form.
Many children are calm, comfortable, and confident in a pediatric dental office. Because pediatric dentists specialize in treating children, they make children feel special. The Papillion Pediatric Dentistry office is especially designed for children. Staff members choose to work in a pediatric dental office because they like children. Sometimes, however, a child feels anxious during treatment. Your child may need more support than a gentle, caring manner to feel comfortable. Nitrous oxide/oxygen is a safe, effective technique to calm a child's fear of the dental visit.
Nitrous Oxide is commonly called laughing gas and is often recommended for children that need to undergo a dental procedure that may be uncomfortable or cause fear or anxiety. The purpose of Nitrous Oxide is to make it more comfortable for your child to receive the necessary dental care with less pain and/or anxiety. Nitrous oxide is classified as an analgesic because it reduces pain and for many procedures makes local anesthesia unnecessary. It is also an anxiolytic, which means your child will be in a pharmacologically induced state of consciousness where he/she is awake but has decreased anxiety to facilitate coping skills, retaining interactive ability. Nitrous Oxide helps to ease patient’s fears so as to help them relax during their visit, and to receive dental treatment in a comfortable and safe manner. It is delivered through a mask over the nose; nitrous oxide is mixed directly with oxygen and delivered as the patient breathes in and out regularly. The patient is usually asked to breathe normally through the nose, and as the gas begins to take effect, the child will become more relaxed and less nervous. It raises the pain threshold and may even make the time appear to pass quickly. Some normal sensations that a patient may feel may include tingling in the fingers, toes, cheeks, lips, tongue, head or cheek area; heaviness in the thighs and/or legs, followed by a lighter floating feeling; resonation in the voice; warm feeling throughout body, flushed cheeks; fits of uncontrollable laughter or giddiness; a lightweight or floating sensation with an accompanying “out of body” sensation; sluggishness in motion and slurring and/or repetition of words. Rarely a child may feel dizzy or nauseous. Laughing gas enhances communication between your child and their doctor during dental procedures. Additionally, it reduces the gag reflex, which can interfere with effective dental treatment. All of these sensations and reactions are temporary and go away after 100% oxygen is delivered at the end of the procedure.
Nitrous Oxide is 100% safe to use during treatment and is eliminated from the body quickly after the gas is turned off. The child will remain awake during the entire procedure and will be able to interact and communicate with the pediatric dentist. After the procedure(s) are over, the nitrous oxide gas will be turned off and your child will be given oxygen for 3 to 5 minutes, which flushes the laughing gas and its effects out of your child’s system. There are no lingering effects. Nitrous Oxide is perhaps the safest relaxant used in dentistry. It is well tolerated, having a rapid onset, and is reversible, can be adjusted in various concentrations and is non-allergenic. Absolutely no one is allergic to oxygen or Nitrogen, which are the only two ingredients in Nitrous Oxide. Your child remains fully conscious and maintains all natural reflexes when breathing the gases. He or she will be capable of responding to a question or request. You should inform our office regarding any respiratory condition that makes breathing through the nose difficult for your child. In a very small percentage of children Nitrous Oxide may not be effective, especially those children who have severe anxiety, nasal congestion or discomfort wearing a nasal mask. We will review your child’s medical history, level of anxiety, and treatment needs and inform you if nitrous oxide is recommended for your child. Dr. Bennett is a Pediatric Dentist that has devoted her entire practice to meeting the dental needs of children.
Sometimes a white composite “filling” is required to restore the esthetics of a front tooth that has sustained a traumatic injury or suffers from one of the many developmental abnormalities that can affect the coloration of adult teeth. Unfortunately, fractured permanent teeth are a common traumatic injury in adolescent children and often requires a simple bonding procedure, which is similar to having a cavity filled, except there is no decayed tooth structure to be removed.
If your child is experiencing a true dental emergency, you can always call our office at (402) 502-1256 and you will be given a number to contact Dr. Bennett directly. We are available to answer to emergency situations for our patients.
Unfortunately, children sustain a fair amount of dental and facial trauma from sports-related injuries, falls and other accidents. The most important thing you can do as a parent is remain calm. If your child knocked out a permanent tooth, timely management is key to maintaining the life of the tooth. Depending on the nature and severity of the trauma, we may be able to effectively treat the traumatic injury in our office or even advise you on the at-home management over the phone (for less severe injuries) until you can make it in to our office. If your child has suffered a true medical emergency that involves more than just the mouth and peri-oral structures, call 911 or bring your child to the Emergency Room of your local hospital.
Reinserting an Avulsed (Knocked out) Permanent Tooth:
1) Find the tooth and do your best to hold it by the crown rather than the root.
2) You may gently rinse the tooth with saline or milk to remove any debris, being careful to only touch the crown of the tooth.
3) NOTE: Do not rinse the tooth with water.
4) If the entire root is still intact, try to reinsert it in the socket. If that is not possible, put the tooth in a glass of milk and take your child and the glass immediately to your pediatric dentist. Please note that baby teeth are generally not reinserted into the socket due to the risk of damage to the developing permanent tooth beneath it, however your child should still be seen by your pediatric dentist promptly.

If your child is experiencing a toothache, first clean the area of the affected tooth thoroughly. Try to dislodge any food particle or debris that might be stuck in the tooth by rinsing vigorously with warm water and using dental floss. You may give your child Tylenol or Motrin/Ibuprofen as directed, but DO NOT place aspirin on the tooth or gums. If the face is swollen, apply cold compresses and call our office immediately. This could be a sign of a serious dental infection that requires prompt treatment.
Valuable time has been reserved for your child’s restorative or hygiene dental appointment. A missed appointment results in lost time, which could be offered to another patient in need of treatment if the proper cancellation notice is given. We make every effort to stay on schedule so we respectfully ask patients to be prompt and keep their appointments. Our standard appointment policy is as follows:
We will attempt to contact you either by phone, text or email prior to your scheduled appointment. This is to confirm with you the day and time reserved for your child.
Please arrive at least 10 minutes prior to your appointment time to fill out any necessary paperwork and update your child’s medical history. If you arrive more than 10 minutes late to your appointment, you may be asked to reschedule. Late arrival for a scheduled appointment leads to inadequate time to accommodate the remaining patients on the schedule. As such, late arrivals of greater than 10 minutes may not be able to be seen depending on the time available. In addition, those patients who are on the schedule and here at the assigned time will be seen first. We will try to accommodate late appointments if time permits.
If you must cancel your child’s appointment, please call our office at least 24 hours in advance. A 24 hour notice is required to cancel or change an appointment. A $55.00 fee may be charged to your account if the appointment is missed, cancelled or rescheduled without 24 hour notice.This fee must be paid before being scheduled again.
Broken or Missed Appointments: If three (3) broken/missed appointments occur or three (3) cancellations without 24-hour notice, our office reserves the right to not schedule subsequent appointments.
Exceptions to this policy can be determined only on an individual basis, according to the circumstances. We understand that occasionally, children’s illness or other unexpected emergencies make it necessary to cancel an appointment with less than 24 hour notice. Please contact our office immediately and we will do our best to accommodate your situation.
For patients without insurance, payment in full is expected for services rendered on that day of service. Major credit cards, care credit, checks, and cash are accepted. Payment plans our available through CareCredit. Please ask for details.
For those patients with dental insurance, Papillion Pediatric Dentistry will send claims to the insurance carrier, provided that the insurance card is presented to the front office at the time of the visit. Dental insurance usually will not cover all of the costs of your child's dental care. Most plans include coinsurance provisions, a deductible, and certain other expenses. Any portion of services not covered by dental insurance along with your deductible is due on the day services are rendered. If there is a balance due after insurance pays that will become your responsibility and is due within 30 days.
Learn more about Insurance by reading the Insurance Facts in the FAQ section of our website
It is important for you to keep us informed of any insurance changes such as policy name, group and id number, or a change of employment. We are not, however, responsible for how your insurance company processes the claims or for what benefits are ultimately paid on a claim. Papillion Pediatric Dentistry bases treatment on your child’s needs, not what your insurance will pay.
Insurance benefit payments are determined by the benefit package that you or your employer purchased. We have no way of knowing if, or what, your insurance company will pay until the actual claim is submitted. Therefore, all account balances which have not been paid are the responsibility of the parent/guardian.
PLEASE NOTE: Many plans have frequency limitations pertaining to various procedures done in our office. These limitations may change from benefit year to benefit year. If you are concerned about coverage for these services, please contact your insurance company prior to your visit. We cannot accept responsibility for negotiating a disputed claim and we allow a maximum of 30-days for your insurance company to clear account balances. We will assist you in dealing with the insurance company, but ultimately the responsibility is with you. If after 30 days, the insurance company hasn’t paid the balance, payment by you will be due in full.
FACT 1 - DENTAL INSURANCE IS A CONTRACT BETWEEN YOU, YOUR EMPLOYER AND THE INSURANCE COMPANY. Papillion Pediatric Dentistry has no influence on what procedures should or are actually covered. The employer and insurance company negotiate the terms ahead of time. We are simply caught in the middle and are not a party to that contract.
FACT 2 – DENTAL INSURANCE DOESN’T PAY FOR EVERYTHING.Unlike medical insurance which often pays a large portion of expenses after deductible or co-payment dental insurance is not meant to be a pay for everything; it is only meant to be an aid to your investment in your child’s dental healthcare. Many common dental services are not even covered by dental insurance.
FACT 3 – FREQUENCIES AND LIMITATIONS OF BENEFITS. The frequency of payment for some procedures may be limited by an insurance company. This is most often encountered in a pediatric dental office with fluoride treatments. The American Dental Association and the American Academy of Pediatric Dentistry recommend the application of fluoride every 6 months since it is proven to be highly effective against tooth decay. Papillion Pediatric Dentistry follows those recommendations to achieve optimal oral health for your child. So, if an insurance plan limits the frequency of the fluoride treatment, the parent will be responsible for this cost. This can also be encountered with other procedures, such as x-rays and sealants.
FACT 4 - MANY INSURANCE PLANS SAY THAT THEY COVER “UP TO 80% OR 100%”. In fact we have found over our decade + in practice that most plans only cover about 50% to 80% of the average total bill. Some individual procedures may pay up to 100% but not the total bill. Some insurance companies pay more, some pay less. The percentage paid is usually determined by how much you or your employer has paid for coverage or the type of contract your employer has set up with the insurance company. The less you or your employer paid for the insurance, the less you’ll receive in insurance benefits.
FACT 5 – BENEFITS ARE NOT DETERMINED BY OUR OFFICE. You may have noticed that most of the time your dental insurer reimburses you or Papillion Pediatric Dentistry at a lower rate than our actual fee. Frequently, insurance companies state that the reimbursement was reduced because your dentist’s fee has exceeded the usual, customary, or reasonable fee (“UCR”) they consider allowable. These allowable fees may vary widely, because each company collects fee information from claims it processes. The insurance company then takes this data and arbitrarily chooses a level they call the “allowable” UCR Fee. Unfortunately, insurance companies imply that we are “overcharging”, rather than say that they are “underpaying”, or that their benefits are low. Generally the less expensive insurance policy will use a lower usual, customary, or reasonable (UCR) figure.
FACT 6 – PAPILLION PEDIATRIC DENTISTRY HAS ONLY RAISED ITS PRICES ONCE SINCE WE OPENED OVER 10 YEARS AGO! If you are paying more for your dental bill than previous years it is because the insurance companies are paying less not because we raised our prices! So please do not blame us for higher dental bills. We do the same work and just receive less money as the insurance companies charge more and pay less.
FACT 7 – DEDUCTIBLES & CO-PAYMENTS MUST BE CONSIDERED. When estimating dental benefits, deductibles and percentages must be considered. To illustrate, assume the fee for service is $150.00 and the insurance company allows $150.00 as its usual and customary (UCR) fee, you can figure out what benefits will be paid. First a deductible (paid by you), on average $50, is subtracted, leaving $100.00. The plan then pays 80% for this individual procedure. The insurance company will then pay 80% of $100.00, or $80.00. Out of a $150.00 fee they will pay an estimated $80.00 leaving a remaining portion of $70.00 (to be paid by you the patient). Of course, if the UCR is less than $150.00 or your plan pays only at 50% then the insurance benefits will also be significantly less.